The Overlap Between ADHD, cPTSD, and Complex Trauma That Most Clinicians Still Miss
You are sitting in yet another clinician's office, trying to explain why you cannot just 'use a planner' or 'practice mindfulness' when your nervous system treats every small stressor like a survival threat. You have been told you have ADHD. You have also been told your ADHD symptoms might actually be trauma responses. Or that your trauma responses look like ADHD. Or that you are just anxious, just depressed, just not trying hard enough. Every professional you see gives you a different primary diagnosis and a different treatment plan, and nothing quite works because nobody is looking at the whole picture. The ADHD cPTSD overlap is one of the most confusing, under-discussed intersections in mental health, and you are not imagining that something keeps getting missed.
This is what happens when three conditions share so many symptoms that even trained clinicians cannot always tell them apart. When your working memory issues might be ADHD, might be dissociation, might be both. When your emotional reactivity gets called 'ADHD impulsivity' in one appointment and 'trauma hypervigilance' in the next. When you have spent years trying to treat one condition while the others keep sabotaging your progress because nobody told you they were there.
Why the ADHD cPTSD Overlap Confuses Everyone
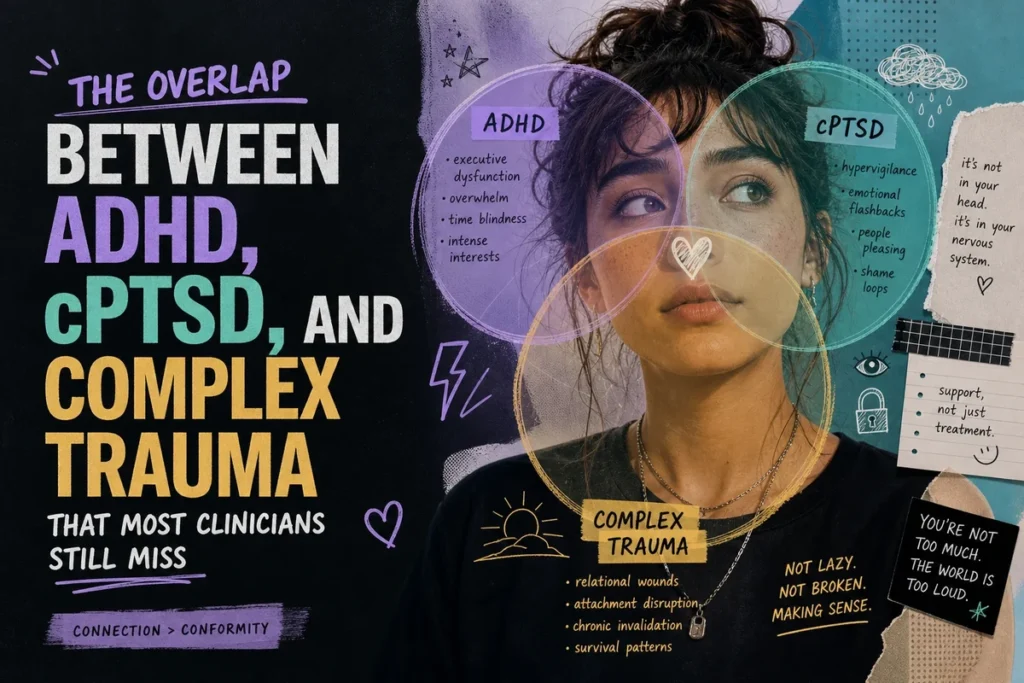
ADHD and complex PTSD share a disturbing number of symptoms. Executive dysfunction. Emotional dysregulation. Difficulty concentrating. Sleep problems. Relationship struggles. Low self-esteem. The diagnostic criteria for these conditions were developed separately, by researchers who were not comparing notes, and the overlap went largely unacknowledged for decades.
Complex PTSD (cPTSD) is not yet a formal diagnosis in the DSM-5, the manual most American clinicians use. It exists in the ICD-11 (the World Health Organization's diagnostic system) and has been extensively researched, but many US clinicians were not trained on it. They know PTSD: the flashbacks, the nightmares, the hypervigilance after a single traumatic event. They may not know cPTSD: the chronic, pervasive effects of ongoing childhood trauma that shape your entire nervous system, your sense of self, your ability to regulate emotions, your patterns in relationships.1
Here is where it gets complicated. ADHD is a neurodevelopmental condition, meaning it affects how your brain developed from birth. cPTSD results from environmental factors, usually chronic childhood trauma, but it also affects brain development. A child who grows up with untreated ADHD in an invalidating environment often develops trauma responses on top of their ADHD. A child who grows up in chronic chaos may develop attention and regulation problems that look exactly like ADHD but are actually trauma adaptations. And a significant percentage of people have both: ADHD brains that are also carrying complex trauma.
When you have been hypervigilant since age six because your home environment was unpredictable, it is genuinely difficult to know if your inability to focus is ADHD or your nervous system scanning for threats. Sometimes it is both at the same time.
The Symptom Overlap That Trips Up Clinicians
Let us look at specific symptoms and how they appear across both conditions.
Emotional dysregulation: In ADHD, this often looks like intense emotions that arrive fast and hit hard, then pass relatively quickly. In cPTSD, emotional dysregulation is often tied to triggers, abandonment fears, and a pervasive sense that your emotions are 'too much' for others. Many people with both conditions experience the ADHD intensity plus the trauma-based trigger sensitivity, creating emotional storms that feel impossible to navigate.
Difficulty concentrating: ADHD attention issues tend to be consistent across contexts (you struggle to focus on boring things whether or not you feel safe). cPTSD concentration problems are often worse when you are triggered, stressed, or in environments that remind your nervous system of past trauma. If you can focus at the library but not at home, that might be environmental. If you cannot focus anywhere, that might be ADHD. If both patterns are true at different times, welcome to the overlap.
Working memory problems: ADHD affects working memory directly. Trauma causes dissociation, which also impairs working memory. The felt experience is nearly identical: you forget what you were doing, lose track of conversations, cannot hold multiple pieces of information in your head. The mechanisms are different, but the result is the same.
Rejection sensitivity: Rejection Sensitive Dysphoria (RSD) is commonly discussed in ADHD communities. But cPTSD also creates intense fear of rejection, abandonment, and criticism, often rooted in early experiences of being rejected, abandoned, or criticized by caregivers. Someone with both conditions may have RSD that is amplified by trauma-based attachment wounds, making social interactions feel like walking through a minefield.
The diagnostic problem: A clinician who only knows ADHD may attribute all your symptoms to ADHD and miss the trauma. A clinician who specializes in trauma may see everything as trauma responses and miss the ADHD. Neither approach gives you a complete picture or an effective treatment plan.
ADHD Complex Trauma Misdiagnosis: The Pattern Nobody Warned You About
ADHD complex trauma misdiagnosis runs in both directions. Some people spend years in trauma therapy for symptoms that are actually ADHD. Some people take ADHD medication for years while their unaddressed trauma keeps undermining their progress. Both scenarios are common, and both are deeply frustrating when you finally realize what happened.
If you were diagnosed with ADHD as a child but grew up in a chaotic, neglectful, or abusive home, there is a real possibility that some of your 'ADHD symptoms' were trauma adaptations, some were actual ADHD, and nobody ever separated them out. The ADHD might have been real AND you might have developed cPTSD on top of it. This is called comorbidity, and research suggests it is extremely common. One study found that adults with ADHD were significantly more likely to report childhood trauma than adults without ADHD.2
The reverse pattern also happens. If you grew up with significant trauma, your symptoms may have been attributed to anxiety, depression, or behavioral problems when you actually had underlying ADHD that was being masked or amplified by trauma. Late discovery of ADHD is increasingly common among people who spent their twenties treating trauma, then realized the executive dysfunction persisted even after the trauma symptoms improved.
The most frustrating part is when treatment for one condition stops working because the other condition is not being addressed. You cannot focus your way out of trauma triggers, and you cannot therapy your way out of dopamine deficiency.
ADHD PTSD Symptoms Similar: A Closer Look
Understanding why ADHD PTSD symptoms are similar requires looking at the nervous system. Both conditions involve dysregulation of the autonomic nervous system, the part of your body that controls fight, flight, freeze, and rest responses.
ADHD involves differences in prefrontal cortex function and dopamine regulation. This affects your ability to regulate attention, impulses, and emotions. Your nervous system may struggle to find a baseline 'calm' state because your brain is constantly seeking stimulation.
PTSD and cPTSD involve a nervous system that has been shaped by threat. Your baseline state may be hypervigilant (scanning for danger) or hypoaroused (shut down, dissociated). Your body learned to prioritize survival over calm because, at some point, survival actually was the priority.
When you have both, your nervous system is working with a brain that struggles to regulate AND a trauma history that taught your body the world is not safe. The combination creates a state that is exhausting to inhabit: always on edge, but also struggling to focus; emotionally reactive, but also sometimes completely numb; desperate for connection, but also terrified of rejection.
Research on the neurobiological overlap is still emerging, but some studies suggest that childhood trauma can actually affect the same brain regions implicated in ADHD, including the prefrontal cortex and the circuits involved in emotional regulation.3 This means trauma may not just coexist with ADHD but may actually make ADHD symptoms worse, and vice versa.
ADHD Childhood Trauma Neurodivergent: The Compounding Effect
ADHD childhood trauma in neurodivergent people creates a specific pattern that deserves more attention. If you grew up with undiagnosed ADHD, you experienced a form of chronic invalidation: being told you were lazy, careless, too sensitive, not living up to your potential. This invalidation, repeated over years by parents, teachers, and peers, is itself a form of relational trauma.
You did not need to experience abuse in the traditional sense to develop trauma responses from growing up neurodivergent in a world that was not built for your brain. The constant message that something was wrong with you, that you should be able to do things you genuinely could not do, creates shame, hypervigilance, and a fractured sense of self that looks a lot like cPTSD.
This is sometimes called 'little t trauma' or developmental trauma, and it is increasingly recognized as a legitimate source of complex trauma symptoms. Your ADHD may have been the first domino. The environment's response to your ADHD may have been the second. And now you are dealing with both the original ADHD and the trauma responses that developed around it.
This is not about blame: Your parents may have been doing their best with the information they had. Your teachers may have genuinely wanted to help. The point is not to assign fault but to understand why you carry both ADHD and trauma, and why treatment for one without addressing the other often fails.
Why This Matters for Your Treatment
The ADHD cPTSD overlap matters because treatment strategies for each condition can conflict with each other if you do not know you have both.
ADHD treatment often involves medication that increases dopamine and norepinephrine. For some people with comorbid trauma, stimulant medication can increase anxiety or hypervigilance because it activates a nervous system that is already in overdrive. This does not mean medication is wrong for you, but it may mean you need trauma stabilization work alongside medication, or that your medication needs to be carefully titrated while monitoring trauma symptoms.
Trauma therapy often involves slowing down, sitting with difficult emotions, and processing painful memories. For someone with ADHD, sitting still and focusing inward can be genuinely difficult. Traditional trauma therapies like prolonged exposure may need to be adapted for ADHD brains that struggle with sustained attention. EMDR (Eye Movement Desensitization and Reprocessing) is sometimes more effective for ADHD plus trauma because it involves bilateral stimulation and does not require you to narrate your trauma in detail.
If you have been trying one treatment approach and it is not working, the overlap may be why. You are not failing at treatment. The treatment may be incomplete.
How to Advocate for Yourself With Clinicians
Most clinicians specialize. They know ADHD, or they know trauma, but rarely both in depth. This means you may need to advocate for yourself to get a complete picture.
When you meet with a clinician, you can say: "I want to explore whether I might have both ADHD and complex trauma symptoms, because I have noticed symptom overlap that does not seem fully explained by one diagnosis." You can name specific symptoms that confuse you: "My concentration problems are worse when I am triggered, but they also exist when I feel calm. I am not sure if that is ADHD, dissociation, or both."
Ask whether the clinician has experience with ADHD cPTSD overlap specifically. If they do not, ask if they can refer you to someone who does, or if they are willing to learn alongside you. Some of the best clinical relationships happen when a clinician admits they do not know everything but is willing to collaborate.
If you are currently seeing a therapist for trauma, you can ask them to assess whether ADHD might also be present. If you are seeing a psychiatrist for ADHD, you can ask them to screen for trauma symptoms. The point is to stop treating each condition in isolation.
You deserve a clinician who understands that your symptoms do not fit neatly into one diagnostic box, and who is willing to create a treatment plan that addresses all of what you are carrying.
Living With the Overlap
Understanding the ADHD cPTSD overlap does not make it easier to live with, but it can make it less confusing. You stop blaming yourself for not responding to treatment that was never designed for your specific combination of symptoms. You start recognizing which strategies help which part of the picture.
Some days, your main challenge is ADHD: the executive dysfunction, the time blindness, the struggle to start tasks. Some days, your main challenge is trauma: the hypervigilance, the emotional flashbacks, the part of you that still believes you are not safe. Most days, it is both, tangled together in ways that are hard to separate.
The goal is not to perfectly categorize every symptom. The goal is to build a toolkit that addresses both, and to find providers who understand that you are not just an ADHD person or just a trauma survivor. You are someone whose brain developed differently AND whose nervous system adapted to survive circumstances that required adaptation. Both things are true. Both things need to be addressed.
The ADHD cPTSD overlap is real, it is common, and it is still under-recognized in clinical settings. Knowing this does not fix anything by itself, but it gives you language for what you have been experiencing and a framework for seeking better care. You are not making this more complicated than it needs to be. It actually is this complicated, and you deserve support that matches the complexity of what you are carrying.
1 Herman, J. L. (1992). Complex PTSD: A syndrome in survivors of prolonged and repeated trauma. Journal of Traumatic Stress, 5(3), 377-391.
2 Biederman, J., et al. (2012). Adult outcome of attention-deficit/hyperactivity disorder: A controlled 16-year follow-up study. Journal of Clinical Psychiatry, 73(7), 941-950.
3 Teicher, M. H., & Samson, J. A. (2016). Annual Research Review: Enduring neurobiological effects of childhood abuse and neglect. Journal of Child Psychology and Psychiatry, 57(3), 241-266.
Rate this article
Was this a useful hit?